Friends, this may be the last article on Basic Common Sense. I fully understand how huge an interest group I am about to touch, and I also fully understand the consequences I may face by bringing this information out. But there is no way, righteousness, I must do it.
If Basic Common Sense disappears, thank you for your encouragement and support.
These days, people are discussing topics such as centralized procurement of drugs and generic drugs. The public and doctors are expressing their concerns, and members of the CPPCC in Beijing and Shanghai have submitted relevant suggestions, reflecting some cases of unstable effects of drugs collected in clinical practice.
In this regard, the National Healthcare Security Administration has always had a firm and clear reply: the drugs collected have all passed the consistency evaluation and have undergone biological risk tests, and their efficacy and safety are trustworthy.
In short, the conclusion of the Medical Insurance Bureau is supported by rigorous scientific experimental data, while the questioning voices are all based on individual observations and subjective guesses.
Is that really the case? Are the data of generic drug consistency evaluation credible?

After Dr. Xia Zhimin’s reminder, on the information disclosure page of the Center for Drug Evaluation of the National Medical Products Administration, I found some experimental data of drugs that passed the consistency evaluation. To be honest, as of the time of writing this article, I have not fully recovered from the extreme shock.
Rosuvastatin calcium tablets, a drug used to treat hyperlipidemia, more than 100 million people in China with three highs (high blood pressure, high blood sugar, and high blood lipids) have to take this drug every day. My mother is also taking it.
Under ideal circumstances, in order for generic rosuvastatin calcium tablets to pass the consistency evaluation and be included in the centralized procurement, they need to be compared with the original research drug (AstraZeneca’s “Crestor”) and conduct a bioequivalence test to ensure that the drug’s metabolic curve in the human body is basically consistent before it can be considered qualified.
Why is it “basically consistent” instead of “completely consistent”? This is determined by the characteristics of drug human trials. The people participating in each trial are different, and each person’s metabolism will be different. Even for the same manufacturer and the same batch of drugs, the data from two trials will only be close, and it is impossible to be completely consistent.
However, the bioequivalence study data of 5mg rosuvastatin calcium tablets from Nanjing Chia Tai Tianqing Pharmaceutical and the data of 10mg rosuvastatin calcium tablets from Lek Pharmaceuticals d.d (Sandoz Pharmaceuticals) are completely consistent.
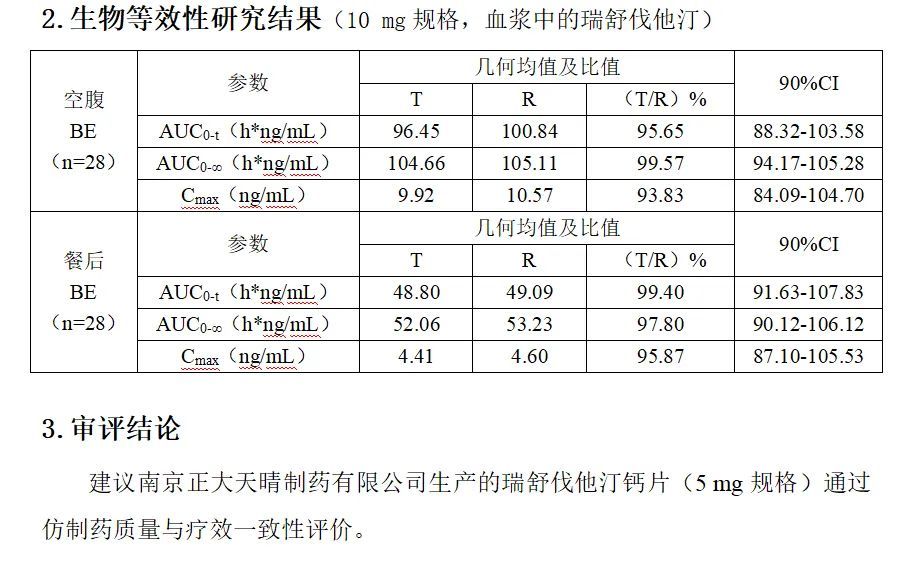
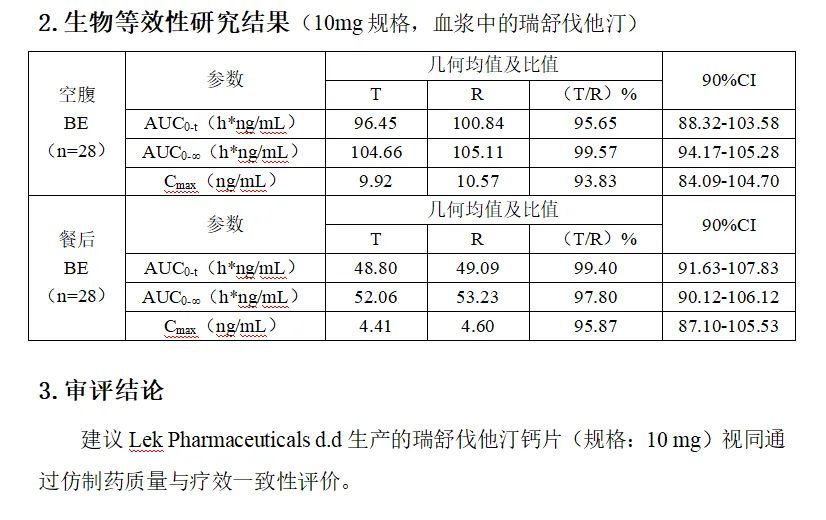
Different drug specifications, different manufacturers, different clinical trial institutions, different subjects, and different trial years, the experimental data are exactly the same, exactly the same to two decimal places.
If the results of the two trials are true, then biology does not exist.
The above data source: https\://www.cde.org.cn/yzxpj
So, is the situation where the BE test data of different manufacturers are completely consistent an isolated case? Could it be that the staff of the Drug Administration made a mistake in entering the data?
Let’s look at another set of data for trimetazidine hydrochloride tablets:
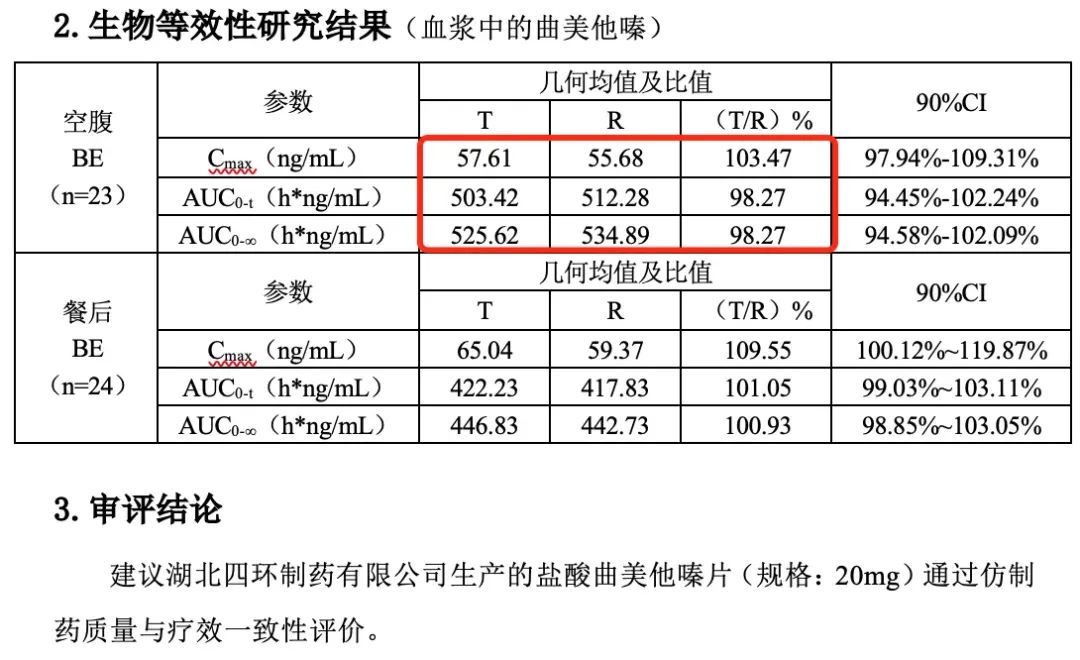
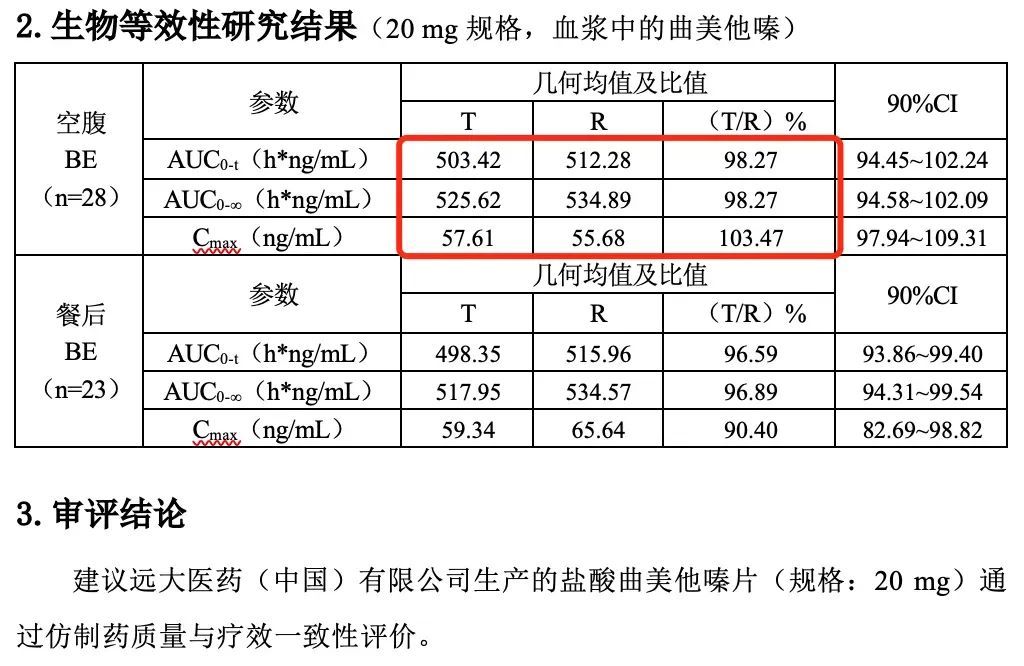
Two 20mg trimetazidine hydrochloride tablets produced by Hubei Sihuan Pharmaceutical and Yuantai Pharmaceutical Company, when taken on an empty stomach, have completely consistent metabolic parameters, which are also completely consistent to two decimal places. However, the metabolic parameters of the two drugs taken after meals showed significant differences.
The above data source: https\://www.cde.org.cn/yzxpj
Because the experimental data are completely consistent, I thought about it for a long time, wondering if it was because of commissioned production, and the commissioning party and the manufacturer used the same set of data to declare separately?
The answer is no.
The four sets of data listed above correspond to 4 different BE test numbers, and even the years are different.
| BE filing number/clinical trial approval number | 2013L00482 |
| BE filing number/clinical trial approval number | B201600005-01 |
| BE filing number/clinical trial approval number | B201900138-01 |
| BE filing number/clinical trial approval number | B201700183-01 |
I repeat:
Different drug specifications, different clinical trial institutions, different subjects, different trial years, the experimental data cannot be completely consistent, absolutely impossible.
Share a personal opinion:
Regarding the centralized procurement of rosuvastatin calcium tablets, which involves 100 million people, if the bioequivalence test is “done” like this, then someone should be shot.
Discover more from 自由档案馆
Subscribe to get the latest posts sent to your email.