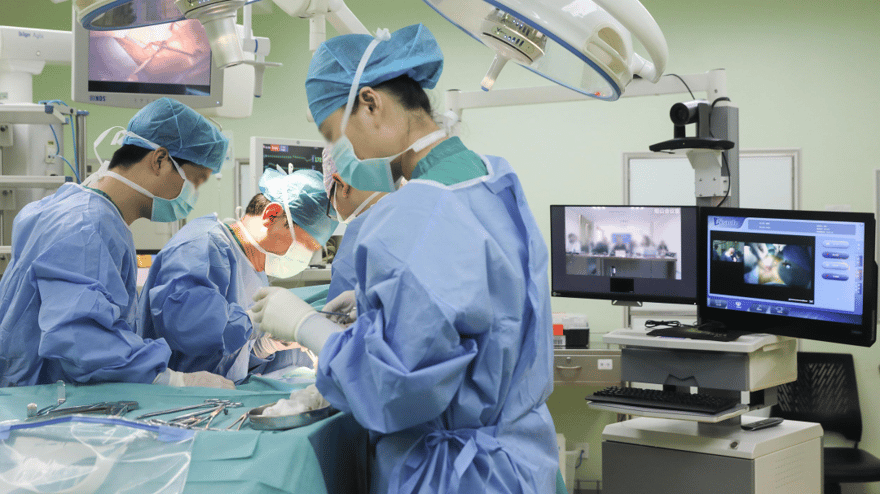
Anze is a resident in cardiovascular surgery. At this moment, he is fighting off the fatigue of a night shift, comparing the expert list with the conference staff to coordinate time points, guest speakers, and content. The conversation in the chat window is rapidly scrolling upwards.
This is his extra work for today, all for the live surgery broadcast tomorrow.
Perhaps because his mentor is a so-called “big shot,” Anze has much more experience in live broadcasting than many senior doctors. From his student days to his current residency, Anze has participated in the live surgery broadcasts of his team for no less than twenty times. “When I first entered school, there were only one or two broadcasts a year. Three years ago, the hospital updated the operating rooms and installed a system that could directly connect to the digital system of academic conferences, and live broadcasts became commonplace.”
However, the live surgery broadcasts, which are essential for domestic conferences and favored by doctors, are strictly controlled in many countries and even banned.
From a new thing to a conference essential
As Dr. Anze feels, any academic conference with a surgical venue, without a live surgery broadcast, seems to mean “lacking weight.”
“From the background data of academic conferences, without live surgery broadcasts, the registration and viewing data will be relatively low.” Chen Jie, the person in charge of the conference, revealed the characteristics of the background data. The medical charity foundation has long supported several large-scale international medical academic conferences.
“I started working on conference affairs in 2015. At that time, most of the academic reports related to surgery used pre-recorded videos. In just a few years, not only have conferences relied on online broadcasts, but live surgery broadcasts have also become an essential part of the program, and they are even heavily promoted in publicity.“
“A conference without live surgery broadcasts is not substantial enough and not high-end enough.” Chen Jie said with a smile, she really wanted to use the word “boosting” to describe the role of live surgery broadcasts in current academic conferences.
Feng Pingzhang, the deputy chief physician of cardiovascular surgery at a tertiary hospital in central China, admitted that he was not surprised that live surgery broadcasts have such a status.
The most basic way to learn surgery is to observe, and live surgery broadcasts can provide more doctors with learning opportunities. At the same time, experts and hospitals at the forefront of technology, in order to better teach and impart knowledge, or to expand their reputation and increase their influence, are very willing to undertake live broadcasts. The needs of both parties coincide on the carrier of “live broadcast,” and the popularity of live surgery broadcasts has become inevitable.
The cardiovascular surgery department where Feng Pingzhang works has very rare opportunities to directly observe top surgeries, and the recorded videos they can find are also very limited: “Although live broadcasts and recorded broadcasts are both videos, the recorded videos are often some classic surgeries, and it is difficult to see the handling of sudden problems after editing, which is only suitable for learning operational norms.”
“The surgeries that are now broadcast live are much newer and the details are closer to reality. For example, the Chinese Heart Conference has had live surgery weeks for several years in a row, with demonstrations of surgeries such as TAVI, and real-time commentary and explanation outside the venue. Although it doesn’t mean that you can do it or have the opportunity to do it after watching it, at least it gives me a learning opportunity.” Therefore, nowadays, if there are live surgery broadcasts when attending meetings and taking classes, it will attract his attention more.
The uneven distribution of medical resources is a chronic disease, both in our country and in the world. Live broadcasts multiply the energy of a demonstration surgery, allowing doctors in different regions to obtain relatively homogeneous learning opportunities. Because of the real benefits, live surgery broadcasts, a new thing, have become commonplace in just a few years.
But as live surgery broadcasts flourish, controversies have also emerged.
British technology philosopher Collingridge once argued: It is very difficult to control a technology, because in its early stages, when it can be controlled, people cannot fully understand its risks, and there is no reason to control its development. But when these consequences become obvious, the cost of control has become very high, and it is difficult to control.
The “Collingridge Dilemma” seems to be gradually emerging in live surgery broadcasts.
Concerns about patient deaths after live broadcasts: may increase surgical risks
In 2004, a patient in Milan, Italy, died after a percutaneous heart valve implantation live broadcast. In 2006, a Japanese patient died after a live broadcast of an aortic aneurysm repair. In August 2015, a Japanese doctor performed a laparoscopic liver tumor surgery live broadcast in India (at this time, the Japanese medical industry association had already banned live surgery broadcasts), and the patient died after the surgery.
Several patient death incidents have raised people’s concerns about the risks of live broadcasts: Will live surgery broadcasts affect the surgeon’s psychology and behavior, leading to a decline in the quality of surgery?
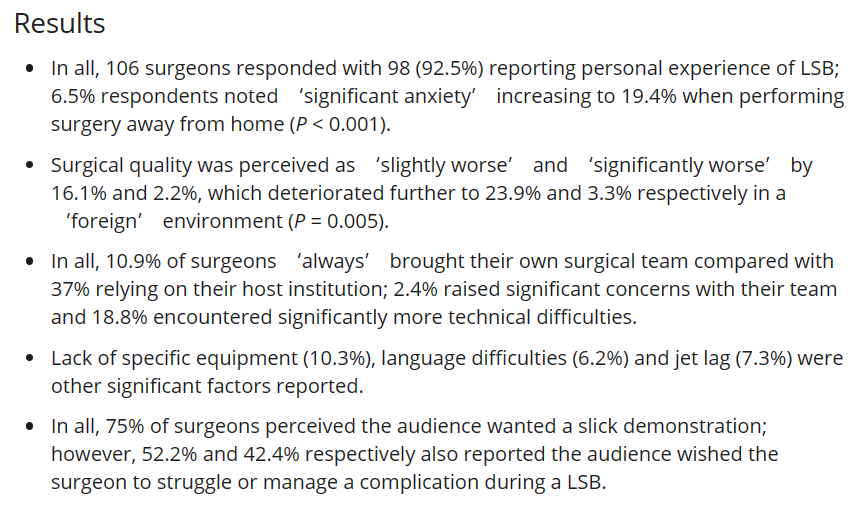
A survey of 106 doctors with live surgery broadcast experience showed that 32.3% of the respondents reported related intraoperative complications. Most respondents (62.4%) admitted to anxiety or worry during the live broadcast, and 18.3% felt that their performance in live surgery broadcasts was not as good as in routine surgery.
Yuan Qing, the deputy chief physician of vascular surgery at a tertiary hospital in North China, said that it is inevitable for doctors to be nervous during the live broadcast, and nervousness may more or less lead to distortion of movements. He further talked about his doubts about performing surgery under the live broadcast camera: “Even if some doctors are not nervous, such as myself, I am more excited, but will excitement distort my operations? This is something I really cannot confirm.”
Yuan Qing believes that perhaps the more top experts are used to live broadcasts and can avoid the impact to a greater extent, but this may really require more research and evidence.
And Dr. Anze, mentioned earlier, said that if the surgery is to be broadcast live, the entire team will have to do a lot more work before and after the broadcast.
Anze feels that it is fortunate that the team members of his mentor are sufficient, and the live broadcast experience is very rich, and the operating room configuration is also complete. “If we also need to adapt to the live broadcast to arrange the surgical procedures and demonstration methods, adapt to the shooting equipment, and arrange the shooting staff, it may also take up the time and energy of the chief surgeon.”
Therefore, Anze has another hidden worry: Will live broadcasts affect the allocation of doctors’ energy, thereby creating surgical risks.
Studies have suggested that frequent interruptions lead to prolonged surgical time, the need to arrange surgical procedures to accommodate conference time, prolonged pre-operative patient waiting time or sudden cancellation of surgery, prolonged anesthesia time, and doctors leaving the surgery early to perform the next demonstration, which increases the risk of patient surgery live broadcasts. Other studies have shown that non-medical technology-related live broadcast communication issues are also significantly associated with adverse events during surgery.
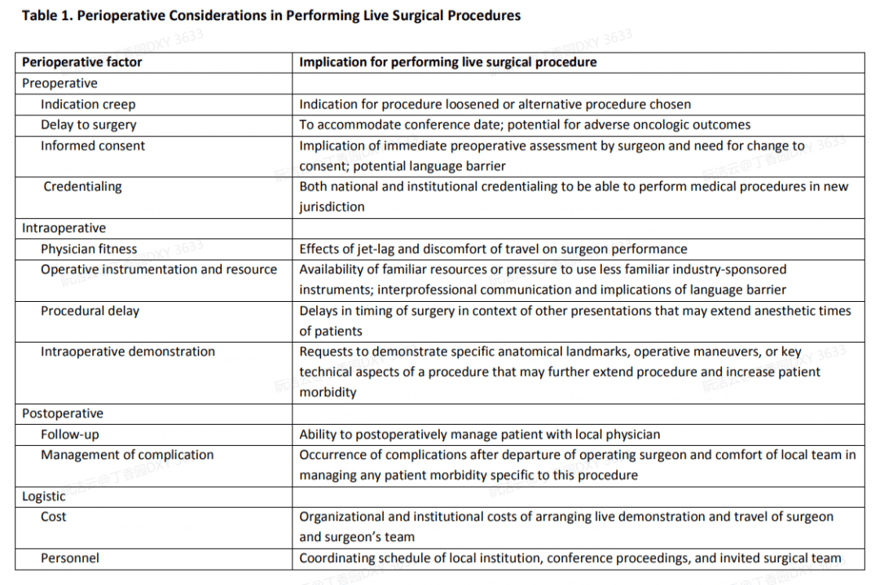
Patients are the bearers of the risks of live surgery broadcasts, and compared to general medical behavior, the risk of infringement of patients’ right to know and consent in live surgery broadcasts is more complex.
For example, the literature points out that when doctors introduce the method and content of the live broadcast to patients before the broadcast, they often induce patients to participate in the live surgery broadcast by reducing the surgery fees and nursing fees, weakening the autonomy of consent; the characteristics of the audience of the live broadcast, the number of people watching the live broadcast are uncontrollable, making it difficult to know; during the live surgery broadcast, doctors will focus on specific parts in order to explain, and these on-site behaviors are often not informed to the patients in advance, increasing the risk of infringement of patients’ right to know and consent.
Multiple countries strictly control or even ban, and our country still lacks norms
In 2006, after the death of the aforementioned Japanese patient after the live surgery broadcast, the medical community was in an uproar, and the Japanese medical community made a rapid response. The Japanese Thoracic Surgery Association and the Urology Association successively banned live surgery broadcasts. In the following years, the American College of Surgeons and the American College of Obstetricians and Gynecologists also issued a ban on live surgery broadcasts.
But as mentioned earlier, live surgery broadcasts do have their undeniable advantages, and a complete ban does not seem to be the best policy. In recent years, some norms have been born abroad to achieve strict management of live surgery broadcasts. For example, the live surgery norms of the European Association of Urology include the following:
Surgeons must be sufficiently skilled and perform a large number of similar cases each year.
Standard cases are more desirable than extreme cases; the patients selected must meet the goals of medical education.
Patient permission must be obtained in advance to conduct live surgery broadcasts, including the time of the surgery; the treatment of the patient cannot be delayed in order to achieve the live surgery broadcast.
The surgeon must submit a detailed preference list in advance, including instruments, disposable supplies and equipment, patient, surgeon and assistant nurse arrangements, etc.
The anesthesiologist must participate in planning the surgical procedure.
In addition, the association also stipulates that live surgery broadcast data must be submitted to the online registration center and complications must be reported using the revised Martin criteria. The association will regularly audit the results to assess compliance and educational role of live surgery broadcasts.
As live surgery broadcasts are emerging and maturing in China, the problem of incomplete laws and regulations is also receiving increasing attention.
During the Fifth Session of the 13th National People’s Congress last year, a representative proposed Suggestion No. 4837: A comprehensive ban on live online broadcasts of surgeries by medical institutions and doctors for non-academic exchanges.
After the suggestion was submitted, the National Health Commission cited the provisions of documents such as the “Basic Medical and Health and Health Promotion Law”, the “Action Plan for Integrity in the Medical Institutions and Their Staff (2021-2024)”, the “Nine Guidelines for Integrity in the Medical Institutions Staff”, the “2022 Key Points for Correcting Unfair Practices in the Field of Pharmaceutical Sales and Medical Services”, and the “Guiding Opinions on Establishing and Improving the Mechanism for the Release and Dissemination of All-Media Health Science Knowledge”.
In March 2023, the article “Improvement and Implementation of the Patient Safety Guarantee System in Hospital Surgery Live Broadcasts” published in “Chinese Hospital Management” more systematically discussed the management and standardization issues of live surgery broadcasts. The article pointed out that from the perspective of Internet supervision, for non-profit medical live broadcast behavior, the platform, personnel, and content of the live broadcast have no specific and clear requirements, only for the inevitable bloody scenes, the existing rules cannot make a direct explanation.
At the same time, in live surgery broadcasts, medical staff, patients, live broadcast platforms, and viewers form a special medical service relationship around patient safety, and the current medical and health legislation does not have special provisions to adjust and regulate the above-mentioned special medical service relationship formed by live surgery broadcasts.
The article further mentioned that there is no unified surgical live broadcast access standard for whether a live surgery broadcast can be carried out, and there is a lack of paradigm. At this stage, 88% of live surgery broadcasts are carried out by industry conferences and sponsored by medical device manufacturers. The process of live surgery broadcasts is chaotic, and it is common for expert judges to arbitrarily interrupt and guide the surgical operations of live broadcast doctors.
In the absence of rules, many hospitals have temporarily introduced some internal norms in the hope of filling the gap in this link, and the hospital where Yuan Qing works is one of them.
“The hospital issued regulations last year that academic live broadcasts and clinical practice teaching live broadcasts have different rules and must be approved internally. Only doctors who have performed a certain number of surgeries using the live broadcast technique are eligible to apply for the live broadcast. At the same time, there are also norms for the selection of patients, such as the need to be assessed as suitable for live broadcast based on the condition, and to fully inform the patient of the scene, audience scope, and broadcast form of the live broadcast, and to sign an informed consent.“
Starting from reality, live surgery broadcasts have their necessity. Having a legal framework, but lacking norms for specific implementation details, may be the most noteworthy issue for live surgery broadcasts at this stage.
References:
[1]COLLINGRIDGE D. The social control of technology”,”. NewYork: St. Martin’s Press, 1980 [M][2]Khan SAA, Chang RTM, Ahmed K, et al. Live surgical education: a perspective from the surgeons who perform it. BJU Int 2014;114:151–158.
[3]Knol Joep,Bonjer Jaap,Houben Bert et al. New Paradigm of Live Surgical Education: Synchronized Deferred Live Surgery.”,”.J Am Coll Surg, 2018, 227: 467-473.
[4]Li Yongwei, Feng Lei. Improvement and Implementation of the Patient Safety Guarantee System in Hospital Surgery Live Broadcasts”,”. Chinese Hospital Management, 2023,43(3):59-62[J] [5]European Association of Urology – Live Surgery Endorsement Guide.
[6]https://www.nhc.gov.cn/wjw/jiany/202211/706c1b8fa5274362a3019fdbc8126d6e.shtml[J].中国医院管理,2023,43(3):59-62
[5]European Association of Urology – Live Surgery Endorsement Guide.
[6]https://www.nhc.gov.cn/wjw/jiany/202211/706c1b8fa5274362a3019fdbc8126d6e.shtml
Discover more from 自由档案馆
Subscribe to get the latest posts sent to your email.